


Ovarian Cyst (Endometriosis)
What is Cyst?
A cyst is a fluid-containing mass surrounded by a tissue called a cyst wall.
Cysts may occur in all tissues of the body, but cysts of organs other than the ovary may show symptoms more quickly. This is because cysts that occur in other organs cause dysfunction in the organs. Generally, this is not the case for ovarian cysts.

What Causes Ovarian Cysts?
The most common cause of ovarian cysts; hormonal disorders.
If the woman has hormonal irregularities, the egg-bearing cysts do not crack and continue to grow to form follicle cysts.
What are the Symptoms of Ovarian Cysts?
Often, ovarian cysts do not show any symptoms. However, symptoms may occur as the cyst grows. Symptoms may include:
- Swelling in the abdomen
- Painful bowel movements
- Menstrual irregularity, spotting or menstruation
- Pain during sexual intercourse
- Pain in the lower back (pelvic region) or thighs
- Breast tenderness
- Nausea and vomiting
How is the Ovarian Cyst Diagnosed?
Usually, during the gynaecological examination, a diagnosis of cyst in the ovary is made by chance. Evaluation by vaginal or abdominal ultrasonography often provides information about the type of cyst and whether it is malignant. Rarely, further investigations such as computed tomography and MRI are needed.
How to Understand Benign Cyst and Malignant Cyst?
Tumour tests in the blood can be performed to differentiate whether the cyst is benign or malignant. Most ovarian cysts are benign. Of these tumour tests, Ca-125 may be elevated, particularly in ovarian cancers and benign chocolate cysts called endometriomas. If the diagnosis cannot be made with all these evaluations, the cyst can be evaluated with a camera by anaesthesia by laparoscopy.
Ovarian Cyst Treatment
If your cyst does not show any symptoms, your doctor can only follow it for 1-2 months. Most functional (functional cysts) resolve spontaneously in one or two months.
If your cyst is large and complains, your doctor may recommend hormone (birth control) therapy or surgery. The form of treatment depends on many factors:
- Size and type of cyst
- Your age
- your complaints
- Your desire to have children
Ovarian Cyst Hormone Therapy (Birth Control Pills)
Your doctor may prescribe birth control pills to treat functional (ovarian) cysts.
Hormones in birth control pills stop ovulation.
This prevents the development of egg sacs and thus stops the formation of new cysts.
Birth control pills may not be suitable for all women, especially for smokers and older than 35 years.
Ovarian Cyst Surgery
Your doctor may recommend surgery to remove the cyst. He will decide which type of treatment is best for you.
The type and size of surgery required to depend on many factors. Sometimes a cyst can be taken when the ovary is released (called a cystectomy).
In some cases, one or both ovaries may need to be removed.
Uterine Fibroids
What are uterine fibroids?
One of every four women is one of the most common problems in women. These are benign masses arising from uterine tissue and protruding from the shape of the uterus.
What Causes Fibroids?
It is known that genetic predisposition is important for the development of fibroids. Most patients have multiple fibroids. Since estrogen causes fibroids to grow, it is observed that they grow during pregnancy, especially during the reproductive age. Fibroids differ according to their placement in the uterus and may grow into the lining of the uterus and may also be present in the intrauterine muscle tissue.
Fibroids, which are still unknown and how they occur, cause pregnancy losses and reproductive disorders. Factors such as age, ethnicity, not having given birth, obesity increase the risk of developing uterine fibroids. In the pathological examinations of the uterus, 77% of women have one or more fibroids and these cause some problems in 60% of reproductive-age women.
What Are the Symptoms of Fibroids?
The most prominent symptoms of fibroids are;
- Too much bleeding during menstrual periods,
- Light bleeding at intervals after menstruation,
- Significant growth in the abdomen and uterus,
- Feeling pain in waist and coccyx after sexual intercourse and menstrual periods,
- Frequent desire to urinate,
- Detailed infertility tests also show that in some cases, fibroids block the tubes.
- Also, fibroids cause constipation due to the pressure they create in the intestine.

How is Fibroids Diagnosed?
Diagnosing fibroids is an easy procedure. For the diagnosis of fibroids; ultrasonography, hysteroscopy, laparoscopy, hysterosalpingography can be used.
Ultrasonography
Ultrasonography, which has been used in the diagnosis of many diseases and problems for many years, is a painless and painless examination method. The internal genital organs are evaluated by images created by sound waves called echoes in the ultrasonography performed with the aid of a device inserted through the abdomen or into the vagina.
Hysteroscopy
Hysteroscopy, ray telescope device with the vagina and cervix neck into the uterus is inserted into the examination process.
Laparoscopy
It is based on a telescopic examination system with a tiny incision in the abdomen of the patient with a device called laparoscope.
Hysterosalpingography
The hysterosalpingography technique is a medicated film technique and is administered by a thin tube that enters the vaginal cavity just inside the cervix. This drug is spread through the uterus through the tubes to the abdominal cavity, and with this medicine, the anomalies in the organs can be visualized more clearly and if any, the anomalies can be diagnosed.
How are fibroids treated?
Because fibroids are usually very small and do not cause complaints, they may not need to be treated. Even some fibroids do not show any symptoms, so the woman may not know that it is fibroids. However, fibroids with severe symptoms, prominent findings, large enough to affect fertility, and can be confused with cancer or similar malignant tumours should be treated. In this respect, if the uterine fibroids are small, it is sufficient to carry out control examinations at intervals of 6 months, whereas treatment of large fibroids is preferred.
Medical treatment
Some drugs called GnRH analogues are used to reduce the size of fibroids. However, when these drugs are used for a long time, they cause bone loss, vaginal drying and hot flashes. For this reason, these drugs are usually used to shrink fibroids before surgery.
Surgical treatment
Surgical removal of fibroids that cause severe complaints and shows rapid growth. The type of surgical application is determined according to the location and size of the fibroid.
Myomectomy
It is the process of simply removing the uterine fibroids from the uterine wall. It is a protective approach that protects the uterus, especially in women who want to conceive, and this procedure is mostly performed with laparoscopy. However, if the uterine fibroid is too large to be removed by laparoscopic procedure, the myomectomy is performed with classical surgery by opening the abdomen.
Hysterectomy (Uterine Removal)
In cases where fibroids grow rapidly and cause too many complaints, hysterectomy is applied to women who do not want a pregnancy in the future.
Follow-up of Fibroids
Small, non-enlarging, non-complaining fibroids do not require surgical removal. Patients with no complaints such as pain, the sensation of pressure, irregular or excessive bleeding should be checked at regular intervals every 6 months to monitor the fibroid size.
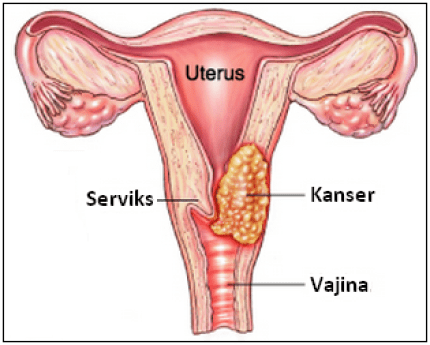
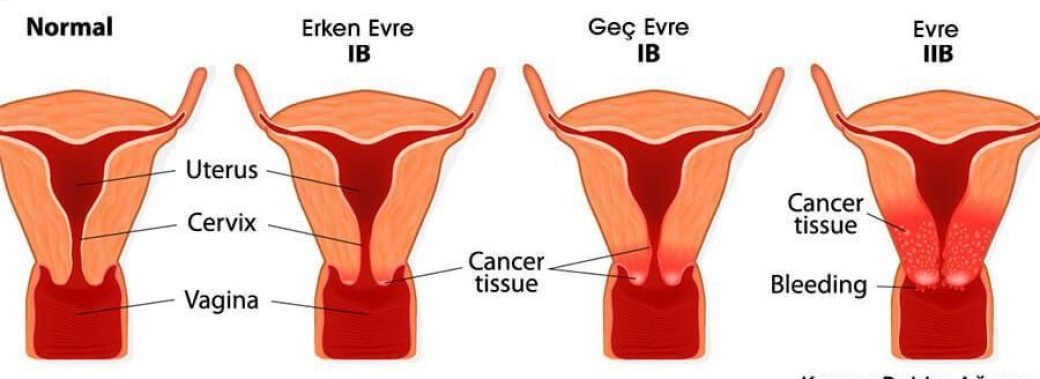
Cervical Cancer (Cervical Cancer)
Cervical cancer, or cervical cancer, as it is called, is seen in the cells in the lower part of the uterus called the cervix. The cervix is the neck-shaped part of the uterus that connects to the vagina. Various types of human papillomavirus (HPV) that cause sexually transmitted infections are the most common cause of cervical cancer.
In most women, when exposed to the virus, the immune system prevents the body from damaging the virus. But in a small group of women, the virus survives for years. These viruses initiate the process that causes some cells on the surface of the cervix to become cancer cells.

What are the Symptoms of Cervical Cancer?
Vaginal bleeding is the most common symptom of cervical cancer. Vaginal bleeding can occur after sexual intercourse or after menopause, except during menstrual periods.
Another common symptom is pain during sexual intercourse. Abnormal vaginal discharge, abnormal breakdown of the menstrual cycle are some of the early symptoms.
In the advanced stage, anaemia develops due to abnormal vaginal bleeding. There is a pain in the lower abdomen, leg and back. The mass may obstruct the urinary tract and cause problems when urinating.
What Causes Cervical Cancer?
Human papillomavirus (HPV) is found in about 99% of cervical cancers. There are more than 100 different types of HPV, many of which are considered low-risk and do not cause cervical cancer. More than 70% of cervical cancer cases are caused by HPV-16 and HPV-18, often called high-risk HPV species. High-risk HPV strains can cause cervical cell abnormalities or cancer.
However, HPV is not the only cause of cervical cancer. Most women with HPV do not develop cervical cancer. Some other risk factors, such as smoking and HIV infection, increase the likelihood that women exposed to HPV will develop cervical cancer.
Cervical Cancer What are the Risk Factors for Cancer?
- Human papillomavirus (HPV) infection is the most important risk factor for cervical cancer.
- Women who smoke are at twice the risk of cervical cancer compared to non-smokers.
- The body is unable to eliminate HPV infections and cancer cells in people with weak immune systems. The risk of cervical cancer increases because of HIV or certain drugs that impair immunity.
- According to some studies, cervical cancer risk is higher in women with chlamydia infection in blood tests and cervical mucus examination.
- Women who do not consume enough fruit and vegetables in their diet may be at risk for cervical cancer.
- Overweight women have a higher risk of developing cervical adenocarcinoma.
- Family history of cervical cancer is another risk factor.

What are the Methods of Cervical Cancer Prevention?
Cervical cancer is one of the few cancers that is almost completely preventable. By avoiding sexually transmitted human papillomavirus, cancer prevention can be achieved to a large extent. A screening test called pap smear is used to prevent cervical cancer before it occurs. There is also a protective vaccine for human papillomavirus. Also, personal precautions such as avoiding smoking, increasing the risk of cervical cancer, eating mainly fruits and vegetables and getting rid of excess weight reduce the risk of cervical cancer.
How Is Cervical Cancer Diagnosed?
If your doctor suspects cervical cancer, or if abnormal cells are found in the cervical screening test, he or she will ask for further tests for further diagnosis.
Colposcopy: This is a tool that allows your doctor to take a closer look at the cervix. It is usually not painful, but you will feel pain if a biopsy is needed.
Needle Biopsy: Needle biopsy from the transition region where cancer cells and normal cells are located may be needed to diagnose.
Cone biopsy: In this procedure performed under general anaesthesia, a small cone-shaped section is removed from the cervix and examined in the laboratory.
What are the Treatment Methods for Cervical Cancer?
Cervical cancer is treated by multiple methods: Loop electrosurgical procedure (LEEP), cryotherapy, laser and conization. These methods are selected and applied according to the degree of the disease.
Methods used to treat cervical cancer:
LEEP: Used in the diagnosis and treatment of cervical cellular changes. It is a method that takes advantage of the effect of cutting and bleeding on the tissue.
Cryotherapy: It is a method that results in cell death by damaging the surface tissue of the cervix by crystallizing intercellular water.
Laser treatment: It can be used in any case where the whole lesion can be seen in spreading cancer and clean as a result of intrauterine curettage.
Conization: The cervix is a surgical method that removes a cone-shaped part from the cervix, which plays a major role in the treatment of cellular changes.
Infertility
What is İnfertility?
Infertility (infertility) is defined as the absence of pregnancy despite 1 year of unprotected intercourse. In 15% of couples, only male-related factors are seen in 20%, both male and female-related factors are seen in 30% and only female-related factors are seen in the rate of not having children. In the 10% pair, there is unexplained infertility. Thus, in 50-60% of couples who have difficulty in having a child, it can be said that a problem in men is partly among the reasons. Although male infertility problems can be understood from a physical examination and sperm analysis, the hormone analysis, ultrasonography and further special genetic tests may be required in some cases.


What are the Reasons for İnfertility in Men?
While 45% causes of female infertility cause, 45% cause of male infertility causes. The remaining 10% is expressed as unexplained infertility. At this stage, in spite of the examinations and investigations, no cause of infertility can be detected. The reasons for infertility in male candidates can be listed as follows:
- Excessive heat or work
- Continuous work
- Problems with sperm morphology
- Congenital or subsequently obstructed sperm channels
- Low sperm count
- No sperm in the semen
- Poor sperm quality
- Exposure to chemicals
- Excessive alcohol and cigarette consumption
The Main Causes of İnfertility in Women:
- Ovulation irregularities
- Closed tubes
- Endometriosis
- Hyperprolactinemia (Milk hormone height)
- Thyroid hormone disorders (goitre, hypothyroidism, hyperthyroidism)
- Pathologies in the uterus (Endometrial ossification)
- Antisperm antibodies
- Surgery on uterus and ovaries
- Previous infections related to genital organs
- Advanced age-related ovarian reserve reduction
- Causes of the cervix, cervical factor
Other Factors that Affect İnfertility:
- Cigaret
- Obesity (Obesity)
- Cervical stenosis (closed cervix)
- vaginismus
- Lack of regular and correct sexual intercourse
- Adhesions in the uterus (Asherman syndrome)
- Luteal phase failure
- Early menopause, early ovarian failure
- To have received chemotherapy and radiotherapy
Infertility Test
In men, this research is carried out with semen analysis. Following sexual abstinence of 3 to 7 days, the sperm sample is examined under a microscope to obtain information on sperm count, motility and structure. Antisperm antibodies may also be added to the tests, if necessary.
The presence of ovulation in women can be understood from the order of menstrual bleeding or can be confirmed by blood tests to be performed 7 days before the expected number. Occasionally, your doctor may want to observe the development of the egg and ovulation for 1 month with ultrasound tests. For the evaluation of egg quality, FSH, LH, estrogen and AMH levels are measured by blood test between the 2nd and 5th days of your period.
Whether the fallopian tubes are open or closed can be controlled by an X-ray film called HSG, or in some cases, it may require a laparoscopy to visualize the inside of the abdomen via telescopic-camera.


How Is Infertility Treated?
In vitro fertilization is the most well-known fertility treatment, but there are different treatment options available to couples who have difficulty in conceiving naturally.
The decision on which method to recommend is based on your age, whether you have had a previous pregnancy, and how long you have been involved in pregnancy, as well as your specific information, after the evaluation of your tubes, egg quality and your partner’s sperm.
Fertility Drugs
If fertility problems arise from the lack of regular ovulation, egg development can be achieved through fertility drugs that can be given in the form of tablets or injections.
While the treatment given in the form of tablets enables the natural fertility mechanisms in your body to work more effectively, the treatment given in the form of injections directly ovaries by stimulating the ovaries.
After each fertility treatment aimed at increasing the number of eggs, the risk of multiple pregnancy increases and, in rare cases, ovarian stimulation called ovarian hyperstimulation may occur.
Vaccination Therapy (Insemination)
This treatment is applied by placing your spouse’s sperm into the uterus with a simple method during the ovulation period when fertility is highest. This method is recommended for fertility problems where the tubes are healthy and the cause is unexplained.
Sperm selected from the sperm sample given by your spouse and the most fertile chances of fertility is passed through the cervix with the help of a plastic tube is left into the uterus.
IVF Treatment
Regular menstrual women form a single egg every month. It is aimed to increase this number with the hormone drugs given from outside in the treatment of IVF.
Although each treatment protocol varies, two parallel hormone therapies are mainly applied to prevent ovulation and prevent ovulation.
In this way, the eggs that reach maturity are collected by a simple needle aspiration method known as cracking needle and fertilized with sperm from the male in the laboratory.
Surgical Methods in Infertility Treatment
Some surgical procedures before IVF treatment increase the chance of pregnancy.
Treatment of endometriosis
- Removal of uterine fibroids, polyps
- Opening of intrauterine adhesions,
- Removal of clogged and enlarged fallopian tubes by accumulating fluid,
- Controlled heat treatment of the ovaries in women with polycystic ovarian disorders and suppressed ovulation
- Surgical extraction of sperm from testis (TESE, TESA) or epididymis (MESA, PESE)
Laparoscopy
With laparoscopy, the instruments inserted through 3 – 5 mm holes in the lower abdominal region can be directly observed and surgical procedures can be performed if necessary.
The cases where laparoscopy is performed are:
- Abdominal adhesions
- Opening of tubes
- Removal of damaged tubes
- Fibroid surgery
- Chocolate cyst surgery
Hysteroscopy
Hysteroscope device can be used to diagnose uterine fibroids, polyps and intrauterine curtain problems and treat them with simultaneous intervention.
The hysterectomy device is in the form of a tube with a camera at its end, extending from the cervix to the uterus, to detect intrauterine problems. Your doctor may take a small sample of tissue if necessary.
Hysteroscopy examination is as follows:
- Intrauterine adhesions
- Removal of masses such as fibroids/polyps
- Intrauterine curtain operation
- Correction of deformities in the uterus
- Observation of uterine cavity
Uterine Sagging
What is Uterine Sagging?
The organs of the genital area have limited mobility due to the ligaments that hold them in place. Due to age progression, several births, the ligaments may lose their function. With the loosening of the ligaments, it is usual for the genital organs to sag into the vagina.


What Causes Uterine Sagging?
- Having multiple births
- Having a normal birth
- Large Baby Breeds
- Advanced age
- Obesity
- Lift heavy load
- Coughing constantly
- Constipation
- Over-strain
What are the Symptoms of Uterine Prolapse?
Symptoms may vary depending on the degree of discomfort of the person. A new sagging problem may not show any symptoms. The main symptoms are:
- Urine and gas leakage
- Frequent urination
- Suffering during sexual intercourse
- Sagging of a part of the vagina
- Pubic, low back and back pain
- Burning while urinating
- Loss of sexual desire
- Constipation
Uterine Sagging Diagnosis
Uterine sagging is usually diagnosed during a pelvic examination.
In case of severe urinary incontinence, a test (urodynamic test) may be required to measure how well the bladder works.
How is Uterine Prolapse Treated?
Treatment depends on the severity of uterine prolapse. Your doctor may recommend:
If you have little or no symptoms of uterine prolapse, simple personal care measures can provide relief or prevent worsening. Personal care measures include Kegel exercises to strengthen your pelvic muscles, lose weight and treat constipation.
A vaginal pessary is a plastic or rubber ring inserted into the vagina to support swollen tissues. It should be removed regularly for cleaning. However, vaginal pessaries have a small use in advanced uterine sagging.
In cases of severe uterine prolapse, your doctor may recommend surgery. Minimally invasive (laparoscopic) or vaginal surgery may be an option.
Surgery May İnclude:
This surgery is usually through the vagina, sometimes through the abdomen. The surgeon may place your tissue, donor tissue or synthetic material in the weakened pelvic floor structures to support your pelvic organs.
Uterine Removal (Hysterectomy)
Hysterectomy may be recommended if uterine prolapse is severe. However, hysterectomy is major surgery, and recent research poses long-term health risks, such as increased cardiovascular diseases and some metabolic disorders.
What Should be Done to Prevent Uterine Sagging?
There are not many methods to prevent this problem. You can only eliminate risk factors. Not doing heavy work, a balanced diet and not gaining excess weight can be an example. You should exercise continuously and keep your doctor’s checks in place.
Pelvic Pain
What is Pelvic Pain?
Pelvic pain is known as chronic pain. It is usually felt in the abdominal region and may be manifested by muscle contraction and cramp-like chronic pain. Pelvic pain can often spread under your back and up to the hip area. In such cases, pelvic pain can cause serious problems.


What are the Symptoms of Pelvic Pain?
- Pelvic pain is usually sudden onset, intense and short-term pain.
- Symptoms include nausea, vomiting, sweating and fever.
- If the pain lasts 6 months or more, it may cause insomnia.
- Constipation decreased appetite
- Symptoms of dizziness and dysmenorrhea
What are the Causes of Pelvic Pain?
- Source of pelvic pain more common in women than men
- usually the lower digestive tract, urinary system, excretory system, nervous system or
- musculoskeletal system.
- Pelvic pain due to gynaecological reasons may be due to non-uterine causes.
- The cause of most pain is psychological.
- The reasons for reproduction can be listed as a miscarriage in pregnancy, ectopic pregnancy, pelvic inflammatory disorders, ovarian cysts, preterm birth.
- Causes of chronic pelvic pain in women related to reproductive organs;
- Severe menstrual pain
- Adenomyosis (uterine thickening)
- endometriosis
- Pains during ovulation (mittelschmerz)
- Ovarian cancers
- Uterine fibroids (noncancerous tumours of the uterus)
How is Pelvic Pain Relieved?
Initially, the real cause of pelvic pain should be found and laparoscopy should be performed if necessary. Infection-related or mass research can be done. The abdomen can be x-rayed by ultrasound and tomography can be performed if necessary. Analgesics and muscle relaxant antidepressants may be recommended as drug therapy.
Uterine Wall Thickening
What is Thickening of the Uterus Wall?
Physiologically, every healthy woman secretes the hormone estrogen with the onset of menstruation, and this proliferation occurs during ovulation and combines with the hormone progesterone to prevent the thickening of the uterine wall.
Endometrial hyperplasia is a tissue that is ejected with bleeding every month during the menstrual period. Thickening of the uterus is a condition that occurs when these hormones do not function normally and cause the inner layer of the uterus to thicken more than normal.
Does Thickening of the Uterus Wall Cause Cancer?
In some cases, excessive balance occurs when the balance between the hormones estrogen and progesterone is disrupted. Since cancer develops from tissues with uncontrolled cell division, this thickening of the inner wall paves the way for cancer.
Who is More at Risk?
- Premenopausal period (over 40 years)
- Long periods between periods
- Obesity
- Diabetes
- Polycystic ovary syndrome
- Use of estrogen-containing drugs
Symptoms of Uterine Wall Thickening
Abnormal menstrual bleeding is the most obvious sign of uterine wall thickening.
The following symptoms may occur:
- Menstrual bleeding is more severe than normal or lasts longer
- Less than 21 days between two units
- Bleeding between two pieces or brown spotting
- Bleeding after menopause
- Hot flashes, excessive sweating, pulse increase
- Vagina dryness, vaginal hypersensitivity, pain in sexual intercourse
- Increase in body hair
Causes Thickening of the Uterus Wall?
Estrogen hormone, which prepares the woman for pregnancy after menstruation, thickens the surface of the uterus. Progesterone hormone, which starts to be produced after a while, acts as a counterbalance and provides balance. The main cause of uterine wall thickening is that the estrogen effect cannot be reduced and this balance is disrupted.


1) Menopause
With menopause, egg production stops and the hormone progesterone is no longer produced. On the other hand, even if there is a significant decrease in estrogen level, the effect that may push uterine thickening may continue. This may also be the case in the premenopausal period.
2) Estrogen Drugs
Estrogen treatments and supplements that are not supplemented with progesterone supplements can cause thickening of the uterine wall. This occurs more frequently in treatments that are used to increase the level of estrogen, especially after menopause.
3) Some Diseases
Hormone imbalances that can be caused by the following diseases can result in thickening of the uterine wall:
- Polycystic ovary syndrome
- Diabetes
- Gallbladder problems
- Thyroid problems
- Rarely, estrogen-producing ovarian tumours
4) Risk Factors
The following factors may increase the risk of uterine thickening:
- To be over 35 years old
- Never get pregnant
- To be advanced to the age of menopause
- Low age at first menstruation
- Being overweight
- Smoke Cigarettes
- One of the family members had ovarian, colon or uterine cancer
How is the Diagnosed?
Ultrasonography
Your doctor may recommend a vaginal ultrasound. Uterine wall thickness is measured in millimetres by ultrasound.
Biopsy
It is the process of removing cells through the uterus with the help of a narrow tube. The cells are examined under the microscope in the pathology department.
Dilatation and Curettage
First, the cervix is enlarged and sample tissue is taken from the uterine wall with a special tool called curette. The tissue taken is examined under the microscope in the pathology department.
Hysteroscopy
It is entered into the uterus with an illuminated thin tubular instrument and the sample is taken from the suspicious areas and sent to pathology. This is done during dilatation and curettage.
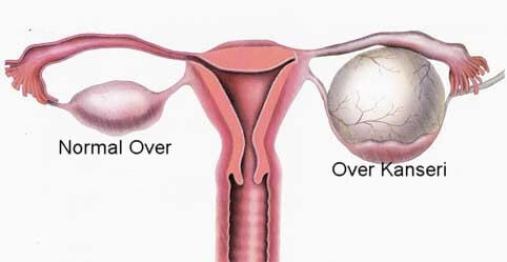
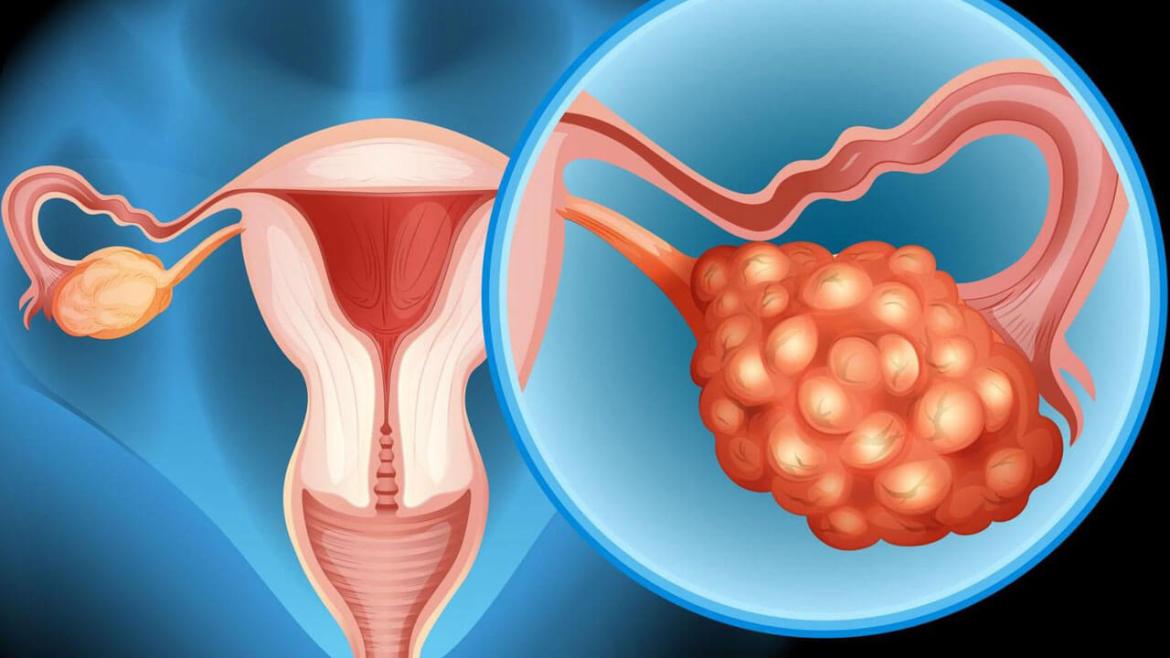
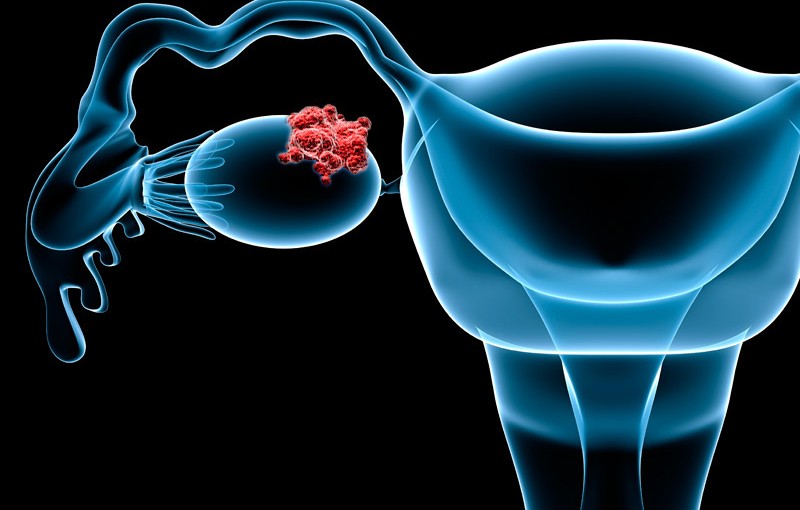
Ovarian Cancer
What is Ovarian Cancer?
Ovarian cancer, the majority of which is seen in the post-menopausal period, 80-90 per cent in the early period with the appropriate treatment, while healing, this rate falls to around 40-50 per cent.
There are many different cells in the ovarian tissue. The tumour is formed as a result of uncontrolled division and proliferation in the epithelial cells or embryonic cells that constitute the main structure of the ovary. Most commonly, epithelial cells arise from tumours.
Epithelial tissue tumours in 80 per cent of people diagnosed with ovarian cancer after menopause, while the detection of people under the age of 20, 60 per cent of the embryonic tumours are detected in the period.

What are the Symptoms of Ovarian Cancer?
Early-stage ovarian cancer rarely causes any symptoms. Advanced-stage ovarian cancer can be confused with benign conditions, as it causes a small number of non-specific symptoms that are more common in benign conditions.
Signs and symptoms of ovarian cancer may include:
- Bloating or swelling of the abdomen
- Quick saturation feeling when eating
- Weight Loss
- Discomfort in the pelvis
- Changes in bowel movements such as constipation
- The need for frequent urination
What are the Stages of Ovarian Cancer?
Ovarian cancer is a disease caused by the excessive division of epithelial cells and other embryonic cells, the main cells in the ovary structure. If the disease occurred after menopause, the deterioration occurred in the host cells. If it was under the age of twenty, the deterioration occurred mostly in embryonic cells. When determining ovarian cancer stages, it is determined how much the disease progresses and whether it spreads to other organs. The stage at which the ovarian cancer is diagnosed is very important. The progression or recovery of the disease depends entirely on it.
Stages of Ovarian Cancer

1: In the first stage, ovarian cancer can occur in only one or both ovaries. However, it has not yet spread to another organ. The first stage is divided into three. At the beginning of the first stage, ovarian cancer is in only one ovary. In the second stage of the first stage, ovarian cancer has spread to both ovaries but has not spread elsewhere. In the next stage, cancer has crossed the ovarian border. A cyst on the ovary may have exploded and the cancer cell can be detected at a location other than the ovary.
2: In the second stage of ovarian cancer, cancer may have spread to other organs in our pelvis. The second stage also has three stages. In the first stage, cancer spread to the uterus and tubes. In the second stage of the second stage, cancer cells can also be seen in the bladder or large intestine. In the last stage of this phase, cancer has now taken any of the first two stages beyond the ovarian border. Also, cancer cells can be seen in the abdominal fluid.
3: In the third stage, cancer spread into the abdomen and involved lymph nodes. In the first stage of this stage, cancer cells can be observed in the abdomen to a very small extent. In the second stage, cancer cells that grow slightly larger are detected as being two centimetres in the third stage.
4: In the fourth stage, the last stage of ovarian cancer, cancerous cells also spread to more distant organs. Cancer cells can also be seen in the liver or lung.
Diagnosis
There is no valid screening method for the detection of ovarian cancer and symptoms are usually
is not remarkable. A protein produced in some ovarian cancers for the diagnosis of ovarian cancer
CA 125, including blood tests and imaging methods such as ultrasound or tomography.
a series of diagnostic tests may be performed.
How is it Treated?
Ovarian cancer treatment usually involves a combination of surgical intervention and chemotherapy.
Surgical İntervention
Treatment usually involves the removal of both ovaries, fallopian tubes, uterus, as well as the removal of the adjacent lymph nodes and folding of the fatty abdomen (omentum), where ovarian cancer is often spread.
If your ovarian cancer is diagnosed at a very early stage, less extensive surgery may be possible. For women with stage I ovarian cancer, surgery may involve the removal of an ovary and a fallopian tube of an ovary. This may preserve the ability to have children.
Chemotherapy
After surgery, you will most likely get chemotherapy to kill the remaining cancer cells. Chemotherapy drugs can be injected into a vein or directly into the abdominal cavity or both.
Chemotherapy can be used as an initial treatment in some women with advanced ovarian cancer.
Childbirth
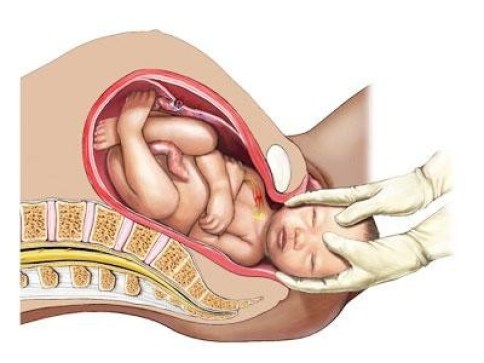
Normal Birth – NORMAL LABOUR & VAGINAL BIRTH
Although birth is a natural process in the female body, the birth of every woman is a unique and special event. There may even be differences between the 2nd and 3rd births of the same mother. Some births occur within one to two hours, while some births may force the mother’s physical and emotional state. Although you do not know exactly how long your birth will last and how it will pass until birth occurs, you may feel more ready by knowing the processes of normal birth.

How is Normal Birth?
There are 3 stages of normal birth. The period from the start of the first regular contractions to full dilatation; The first stage, the time from full dilatation to the birth of the baby, is the second stage and the third stage is the separation of the placenta.
How is Normal Birth Done?
Stage one:
The cervix begins to open with the birth pains coming regularly every 8-10 minutes. The mucus plug that covers the cervix is excreted in a slightly bloody manner. The first stage of labour is the longest stage of labour. Approximately 85-90% of the entire delivery time passes in the first stage. The patient should not be tired at this stage.
In this phase, you can do some activities that will relax you. These are briefly;
- Taking a light walk
- Taking a warm shower
- Relaxing listening to music
- To apply relaxing breathing techniques taught in childbirth education
- Change position
When the cervix opens approximately 6-7 cm and the baby’s head presses the entrance of the birth canal fully, the water sac opens. Once the water sac is opened, the intensity of the pain is slightly reduced due to the decrease in the tension in the uterus, but then increases again.
Second Phase:
When the cervix is fully opened, birth has started. At this stage, the pains have increased and are now at the highest level. Pains come in 2-3 minutes apart and continue for 60-70 seconds. At this stage, the mother begins to feel an uncomfortable strain in the will along with the pain. This period lasts for approximately one hour for the first child and half an hour for the second or third child. The prolongation of this period is important for the health of the baby. This is why the baby’s heartbeat is often rested.
Third Stage:
At this stage, the expectant mother is now relieved and holds her baby in her arms. Some hospitals allow the mother to breastfeed at this stage. The mother’s attention is now shifting to her baby, but many events continue to occur at this stage. The placenta, which provides the whole connection of the baby to the mother, is still in the womb.
After the placenta shows signs of separation, the placenta is removed by massaging the uterus from the top. This phase does not exceed half an hour. When the placenta exits, you may need to push one last time. After the placenta comes out, the vagina and the vagina are checked and sutured if any tears occur. It is also checked by the doctor to see if the placenta comes out in one piece. By controlling the patient’s bleeding, delivery is completed.
Symptoms of Normal Birth
There are many symptoms of normal birth. Not all of these symptoms are observed in mothers. For example, some symptoms, such as engagement, may not be noticed or appear at all.
Symptoms of normal birth; bloody discharge called regular sightings, regular contractions, the arrival of water, back pain, feeling of relief, energetic and happy feeling, frequent urination needs.
- Engagement (bloody discharge): To protect the baby from infections in the womb, there is a mucus plug in the cervix. With the baby coming down and the birth approaches, this plug is discarded with some blood.
- Regular contractions: Regular contractions are the most reliable predictors of the onset of labour. You can change the position to understand the difference between true labour and false labour. If the pains do not disappear or the contractions become more frequent and more severe, this is the real labour pains.
- Water arrival: The baby is found in the womb in a pouch filled with a liquid called amniotic fluid. Amniotic fluid flows when the sac of the sac is torn with pains. This event is called the arrival of water. Even if you have water, but do not show any other symptoms, you should consult your hospital as soon as possible.
- Back pain: Muscles that start to contract and stretch for birth can also affect your back muscles. Therefore, sometimes in some pregnant women before birth pains can be observed markedly back.
- Feeling of lightness: With the baby’s head sitting in the birth canal, the mother’s belly is observed lower. As the infant descends no longer presses the lungs as much as before, a feeling of relief occurs in the mother.
- Frequent urination: As a result of the baby coming down, the urinary bladder will tighten and the mother’s desire to urinate will increase.
- Feeling energetic and happy: Some mothers feel energetic and happy just before birth begins.
What Week Does Normal Birth Occur?
Normal delivery occurs between 38th and 40th weeks of pregnancy. Births before 37 weeks are called preterm births and births after 42 weeks are called late births. Some of the birth symptoms listed above can occur even 4 weeks before the baby arrives. The best physician decides when normal birth begins.
Benefits of Normal Birth
- It causes the mother and the baby to carry out a healthy birth without risking the health of the baby. Everything is natural, as the name suggests.
- Cesarean section, which is often preferred today, is not a method that can be chosen instead of normal birth. Cesarean section is the method used in cases where it is dangerous to perform under normal conditions.
- There will be no need for anaesthesia since surgery will not be performed in the normal delivery method.
- After the birth of the baby, the risk of bleeding and infection will be minimized.
- Hospital stay will be reduced, they can recover quickly and go home.
- Mothers who are conscious because they will not get anesthesia can breastfeed their babies more easily and smoothly.
- According to the studies, babies who will be born with normal birth will pass through the birth canal and encounter some beneficial bacteria and strengthen the immune system.
Here Are The Benefits of Normal Birth For The Baby:
- When the baby enters the birth canal during normal birth, he/she experiences his / her first meeting with the bacteria. This meeting is thought to have a very important place in the baby’s immune system.
- After a normal birth, the mother and the baby meet more quickly, which is important for initial attachment.
- Babies born with a normal birth can be fed faster because the milk comes from the mother faster after a normal birth.
Cesarean Section
What is Cesarean Delivery?
If vaginal delivery does not occur due to various reasons, the operation of the baby to be born through an incision in the abdominal region is called cesarean delivery. This method of delivery, which is often referred to as caesarean section, usually does not exceed 1 hour. Now let’s focus on all your curiosity about cesarean delivery.
It is the operation of the birth of the baby in the womb through a surgical operation. Normally, the cesarean delivery, which lasts between half an hour and forty-five minutes, may take up to an hour when small disruptions are encountered. Unlike normal birth, the anaesthesia used during cesarean section is twice as intensive as the anaesthesia used during normal birth.


A previous cesarean delivery is planned at the 34th week of pregnancy and after. The development of the lungs of infants before the 34th week was not fully completed. For this reason, caesarean delivery is not appropriate before the 34th week. The baby born before cesarean section before 34th week is very likely not to survive.
Why Choose Cesarean Section?
- Large baby and the possibility of damaging cervix during delivery
- Assuming that the baby is not in the ideal position for childbirth
- Having a medical condition that may cause difficulties or complications in normal birth
- Doubt or concern that this birth will be difficult by looking at previous births
- Personal preference – some women who want to give birth at a time that is appropriate for maternity leave or the date of birth, prefer to give birth by caesarean section
- Avoiding normal birth pain and vaginal damage
- Expect triplets, quartets or more.
Caesarean section is a surgical procedure performed under local, general or epidural anaesthesia and as with all surgical procedures, it carries some risks for mother and baby. Some of these risks are listed below:
- Risks arising from anaesthesia and possible allergic reactions to anaesthesia
- If the date is incorrect, the baby’s unplanned preterm delivery increases the risk of the baby’s respiratory problems.
- Respiratory distress syndrome, defined as fluid retention in the lungs of the baby (natural birth removes the fluid filling the lungs while the baby is still in the uterus.
Types of Cesarean Section
Epidural Cesarean Section


Children born by cesarean section are removed from the uterus surgically, not from the mother’s womb. Caesarean delivery is usually preferred when normal birth will endanger the health of the mother and the baby. The debate on hazard risk assessment continues.
Cesarean section is usually performed under epidural anaesthesia (or spinal block). In epidural cesarean section, the mother’s consciousness is clear during delivery. The mother doesn’t feel the pain of the surgery. However, in some cases, the anaesthetist may prefer to use general anaesthesia.
With developing technology, cesarean delivery is considered very safe. But experts say cesarean delivery is less safe than a normal birth.
Elective Cesarean Section
Normal birth can sometimes pose a risk to the mother and baby. In such cases, doctors may recommend caesarean delivery to the mother. Ultrasound scans during pregnancy can reveal the reasons for planned caesarean delivery. Together with these reasons, surgery can be planned before the mother’s labour pains begin. This pre-planned operation is called an “Elective Caesarean Section”.
In Which Situations Can We Choose Elective Caesarean Section?
- If the baby has a known high-risk condition and needs to be born immediately,
- If the mother has a known high-risk condition (pre-eclampsia or placenta Previa), or if she carries a disease that can infect the baby during delivery, such as HIV +, Hepatitis or genital herpes,
- Baby is upside down (feet in front) or transverse (sideways) and enters the pelvis too deep to be rotated,
- There are three or more babies (and usually twins),
- Mother has had a previous cesarean section or has had uterine surgery, elective caesarean section is recommended.
Emergency Cesarean Section
During normal delivery, sometimes things don’t go the way we want. Complications may occur or the doctor may be at risk for the mother or the baby. To reduce this risk, it can be administered suddenly until caesarean section. This is called “Emergency Cesarean Section.
In which cases is an Emergency Cesarean Section Decided?
- Baby becomes distressed during delivery and needs to be born quickly,
- If the mother’s health deteriorates during delivery (eg sudden blood pressure increase, fatigue, preeclampsia or other causes),
- Very rare, but extremely serious problems, such as cord sagging (in the absence of oxygen to the infant whose umbilical cord is compressed) or uterine rupture (if not so medical, can we write it more clearly and in folk language)?
- If the baby enters the uterus in a position that makes it difficult or dangerous to give birth.
- There is a long-term pregnancy that does not show any progress, normal birth can immediately turn into the caesarean section.
Birth in Water


What is Birth in Water?
In a birth pool or tub designed specifically for birth, births in water are called births in water. Not only to be in the water at the moment the baby is born, but also to benefit from the relaxing effect of water to meet contractions more easily during the birth process.
How to Give Birth in Water?
After birth begins, the birth pool or tub is filled with warm and clean water. As it cools, the environment may need to be heated by adding hot water to the water. The mother who relaxes in the water during the contractions can also stay in the water at the exit of the baby if she wishes.
Benefits of Birth in Water
- Research shows that mothers who give birth in water need medical interventions at birth (like pain, epidural, episiotomy) less.
- Being in warm water provides a sensual relief and increases the secretion of oxytocin hormone. When enough oxytocin is secreted during labour, contractions become more regular and delivery time can be shortened. A more positive, calmer birth experience is possible.
- Another effect of warm water is that it softens the muscles and tissues and reduces the feeling of pain and tension. Especially with the softening of the muscles in the abdomen and groin can ease birth.
- Being in the water gives a psychological feeling of trust and the mothers who feel safer can feel more comfortable, free and strong during childbirth.
- Developed in an environment full of water for 9 months, the baby is born into warm water can experience a softer transition. It is observed that babies born in water are a little calmer than other babies.
What are the Conditions to be Fulfilled for Birth in Water?
- The family must have a professional preparatory training before birth. Birth in water is a natural birth. The family should not be panicked should be provided with a peaceful environment.
- Full communication and trust should be established between the mother and the health personnel in the water.
- The mother should be a suitable candidate for birth in water. Risky pregnancies are not suitable for birth in water.
- Professional supporters of the family should be educated and willing about natural birth.
- The hospital should have adequate personnel and training for emergencies.
In What Situations is Birth in Water Risky?
- When the necessary environment is provided, the risk of birth in water is not more than the risk of birth. Also, with the water calming both individuals, the birth process is easier than usual.
- If the baby is reversed, water birth may be risky.
- The baby is too large, water birth may be risky.
- Mother has diabetes, water birth is not recommended.
- The mother is going to give birth to twins or more babies, water birth may be risky.
- If the temperature and disinfectant of the tub or pond to be delivered cannot be adjusted well, water birth may be risky.
- Mother’s faeces are contaminated with water, germs in these faeces can infect the baby.
- Waterbirth brings the risks of infection as the birth canal is open at birth.
- Birth in water does not promise painless birth to the extent that the epidural provides.
- The mother has excess weight, water birth can be risky.
- Preterm labour is not recommended in water.
Epidural Birth
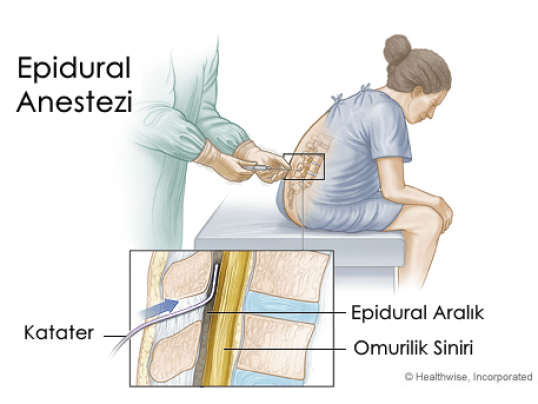

What is Epidural Birth?
In epidural birth, an anaesthetic is given through a catheter inserted into the spinal cord by entering with a special needle from the waist of the mother before birth. This application aims to numb the waist down and prevent pain from being felt. Other names include painless delivery and epidural analgesia.
Painless birth is a method used for normal birth. However, in cases where normal delivery started with this method cannot be performed for any reason, the caesarean section can be performed by increasing the dose and concentration of drug given from the waist-inserted epidural catheter.
How is Epidural Birth Performed?
The epidural method is applied after the uterine contractions become regular after thinning the cervix approximately 60-70%, and the opening reaches 4 cm, ie when the pains start to seriously disturb the mother. Epidural anaesthesia before this stage affects contractions and delays birth. When the patient is late, both the mother suffers unnecessary pain and the pain will be more frequent and the mother cannot remain still during the procedure and epidural administration may be difficult.
After the application of the drug warming and tingling of the feet begins, and then drowsiness up to the level of the belly is felt. The administration of epidural anaesthesia lasts approximately 10 minutes, while the pain begins to diminish shortly after administration. It may take up to 15 minutes for the epidural to fully feel the effect. When the pain is exacerbated by the progression of labour and the decrease in the effect of the drug, the dose is adjusted again by the specialist physician.
What are the Advantages of Epidural Birth?
The epidural method is a normal delivery without pain. In this method, alleviating birth pains has a positive effect on the health of the baby and the mother and greatly improves the comfort of birth. As the mother does not get tired or feels pain during the birth process, she can easily push and actively participate in labour. When the mother gives birth to her baby, she enjoys that beautiful moment because she is awake and painless. After birth, the mother will soon be able to take care of her baby and breastfeed. This method does not apply a large number of negative effects on the mother and baby is very little.
Advantages of Epidural Anaesthesia can be Listed as Follows;
- This anaesthesia provides highly effective pain control during normal delivery and can be administered throughout the entire delivery process.
- It helps the mother to rest during long term births and to be able to store the necessary energy to be able to push strongly during birth.
- It makes it possible for the mother to have a positive birth experience by disabling the negative aspects of birth.
- Thanks to epidural anaesthesia, the mother can play an active role in the entire delivery process and can witness every moment of birth.
- Unlike systemic anaesthesia drugs, only a very small dose of the drug is transferred to the baby. Epidural birth is a very safe method for both mother and baby.
- Epidural anaesthesia provides an easy transition from normal birth to the caesarean section in emergencies.
- This Tecnic is also possible for the mother to recover easily after birth and to take care of her baby immediately.
Birth with Spinal Anesthesia
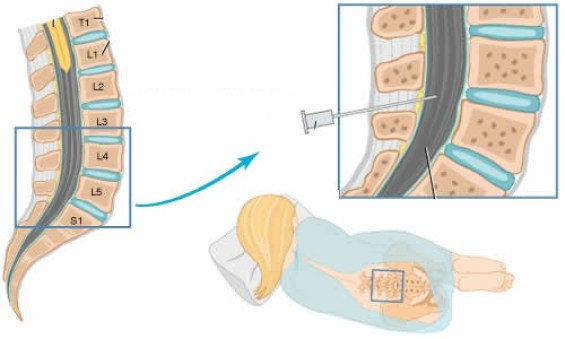

What is Spinal Anesthesia?
Spinal anaesthesia is one of the anaesthesia methods that awake during cesarean delivery and allows to see the baby immediately after birth. It is a type of anaesthesia which is applied only in caesarean section, where the medication given from the waist is anaesthetized for painless delivery. Cesarean section is performed under general anaesthesia by sleeping the patient. Those who do not want this method, the so-called anaesthesia below the waist to apply anaesthesia techniques. In addition to spinal anaesthesia, epidural anaesthesia, which offers the same method, is one of the most confusing types of anaesthesia.
What is the Difference Between Spinal Anaesthesia and Epidural Anaesthesia?
- Both anaesthesia methods are the same. Both are made from the spinal cord to numb the waist down.
- However, in epidural anaesthesia, the drug is injected out of the membrane around the spinal cord, whereas in spinal anaesthesia, this membrane is passed and administered to the fluid in it.
- After epidural anaesthesia, the numbness sensation lasts for 10-15 minutes, while spinal anaesthesia begins immediately or 1-2 minutes later.
- The duration of epidural anaesthesia can be prolonged by re-injecting the drug, but spinal anaesthesia is administered only once, but not.
- During epidural anaesthesia, a thin catheter is located on the waist of the expectant mother during the operation and additional dose is given if necessary. In spinal anaesthesia, the drug is given by injection and removed, no catheter is present.
- Epidural anaesthesia may be preferred by cesarean section or normal delivery.
- But spinal anaesthesia can not be done by those who will give normal birth.